

Groin Injury
At Groin Pain Clinic, all hernia repairs and groin reconstructions are done without the use of hernia mesh.
Injury to the groin is a very common sporting injury and may occur in about 25-50% of elite athletes. Long-standing groin pain without a detectable hernia is termed occult hernia, sports hernia or athletic pubalgia or osteitis pubis, and often doesn't respond to conservative treatment with physiotherapy and rehabilitation.
A wide range of sports and activities which require repetitive twisting, turning and kicking movements can cause these injuries. These injuries are not frequently seen in women, but 10% of cases have been encountered in females. The typical patient will often have had ongoing groin pain for often between 2-3 years before getting something done about it. There may be co-existing injuries of tendons, nerves and bone.
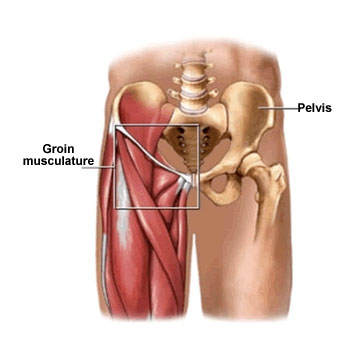
Groin disruption injury occurs in those who participate in sports involving quick acceleration/deceleration, swift change in direction and kicking. Chronic bone stress and wear & tear causes degeneration of the midline pubic bone joint (symphysis).
Instability of the pelvis, on a background of soft tissues that insert into the body of the pubic bone become dysfunctional and disrupted resulting in a sports hernia or footballers groin injury.
History
The onset of pain is usually gradual, but in some sports such as touch football, a sudden injury from slipping on a moist grass surface or during a specific tackle or ruck can cause a sudden disruption. The pain is typically well localised to the area around the pubic bone and pain is often also described in the region of the Adductor tendon insertion with radiation to the testicle or to the other side and also around the bottom area (perineum).
Examination
Physical examination usually demonstrates pain in the pubic area and lower abdomen on resisted sit-up. Squeezing the knees against the examiner’s fist (Adductor squeeze test) may also be a prominent positive physical sign. Seldom is there a positive cough impulse to indicate that a hernia is present.
Radiology
Erect weight-bearing plain X-rays of the pelvis with single leg standing (flamingo view), ultrasound, dynamic CT scanning and Magnetic Resonance Imaging (MRI) scan are all reliable forms of diagnostic imaging. Herniography is not favoured because of the incidence of false negative results and because of the risk of accidentally sticking a needle into the intestines. Sometimes radionuclear bone scan is necessary to confirm the diagnosis of osteitis pubis.
New patients are encouraged to have a specialist groin ultrasound before consultation at the Groin Pain Clinic. Dr Garvey recommends the services of Dr James Black and Dr John O’Rourke, the Principal Radiologists at Medscan Double Bay & Medscan Barangaroo.
Treatment
Surgical treatment is usually only considered after a three to six month trial period of non-operative treatment in the hands of a specialist Sports Physician and / or a dedicated groin physiotherapist. About 20% of patients will show some improvement within a six month period and may not need surgery.
Surgical Techniques
The surgery is a complex variant of the standard open hernia repair (not "key hole"), which involves gathering of deep fascia with a blanket stitch, and a darn repair of the muscles of the posterior wall of the inguinal canal. Other injuries such as a conjoint tendon tear may need to be repaired by sutures placed along the pubic crest (Hyde technique) and release of a torn or damaged Adductor tendon may also be combined with the hernia operation. Occasionally release of the entrapped Obturator or lateral femoral cutaneous nerve will be also necessary. Inguinal hernia repairs are performed using Moloney Darn or the Desarda technique which is mesh free and tension free. Dr Garvey also offers the Shouldice repair, which is another surgical technique for mesh free repair. Dr Garvey also offers reconstruction for recurrent Desarda hernia repairs in addition to Desarda repair for primary hernias.
All hernia repairs and groin reconstructions are done without the use of hernia mesh.
For more information, please read:
Are current techniques of inguinal hernia repair optimal? A survey in the United Kingdom.
Morgan M, Reynolds A, Swan AV, Beech R, Devlin HB. Annals of the Royal College of Surgeons of England. 1991 Nov;73(6):341.
Randomised controlled trial of laparoscopic versus open repair of inguinal hernia: early results.
Lawrence K, McWhinnie D, Goodwin A, Doll H, Gordon A, Gray A, Britton J, Collin J. BMJ. 1995 Oct 14;311(7011):981-5.
Shouldice's herniorrhaphy versus Moloney's darn herniorrhaphy in young patients (a prospective randomised study).
Thapar V, Rao P, Deshpande A, Sanghavi B, Supe AN. Journal of postgraduate medicine. 2000 Jan 1;46(1):9.
Success Rates
Our published success rate for surgery is 94%. There is one prospective randomised control trial published from a Swedish Centre which shows that patients who underwent surgery had significantly less pain when jogging, sprinting and kicking than patients managed by physiotherapy or individual strength training.
Post-Operative Rehabilitation
Enthusiastic commitment to rehabilitation enables return to sport between 8 to 12 weeks after surgery. In the first few weeks, power walking, stationary cycling and swimming are all that is recommended. Thereafter, the Sports Physician or Physiotherapist takes over with a specific treatment protocol. Preventative physiotherapy for players who are at risk of groin injury is encouraged and certain strategies have been devised which consist of the use of the Swiss ball for increasing flexibility and strength of muscles arising from or acting across the hip joint, concentrating on symmetrical conditioning and stabilising abdominal pelvic muscles are encouraged.
Northern Sports Physiotherapy Clinic provides a 3 month guide for those who have no existing management plan in place. Dr Garvey also works closely with the physiotherapists at BaiMed Physiotherapy & Sports Injury Clinic in Wollongong and the Illawarra, Aspire Physiotherapy Centre on the Central Coast as well as Bondi Physiotherapy & Sports Injury Centre and City Edge Physio in Sydney.
Groin Pain Definition
- Groin pain that persists for 6 months (including elite athletes with access to high level care) despite compliant treatment by a Sports Physiotherapist (with a specific interest in soft tissue groin injuries).1
- Associated with a structural injury i.e. "abdominal wall muscle tear demonstrated on ultrasound should be evaluated for surgery as soon as practical".2
1. HOGAN, A (physiotherapist) personal communication
2. Eur. I. Sports Traumantel. Rel res. Vol 2 3 (4) Dec 2001
8:30 am - 5:30 pm
Monday - Friday
GENERAL ENQUIRIES
contact@groinpainclinic.com.au
MEDICO-LEGAL REFERRALS
garveydirect@groinpainclinic.com.au
FAX +61 2 9004 1059